Vitamin D is a group of fat-soluble secosteroids responsible for increasing intestinal absorption of calcium, magnesium, and phosphate, and multiple other biological effects.[1] In humans, the most important compounds in this group are vitamin D3 (also known as cholecalciferol) and vitamin D2 (ergocalciferol).[2] Cholecalciferol and ergocalciferol can be ingested from the diet and from supplements.[2][3][4] Only a few foods contain vitamin D. The major natural source of the vitamin is synthesis of cholecalciferol in the skin from cholesterol through a chemical reaction that is dependent on sun exposure (specifically UVB radiation). Dietary recommendations typically assume that all of a person's vitamin D is taken by mouth, as sun exposure in the population is variable and recommendations about the amount of sun exposure that is safe are uncertain in view of the skin cancer risk.[5]
Vitamin D from the diet or skin synthesis is biologically inactive; enzymatic conversion (hydroxylation) in the liver and kidney is required for activation. As vitamin D can be synthesized in adequate amounts by most mammals exposed to sufficient sunlight, it is not an essential dietary factor, and so not technically a vitamin.[4] Instead it could be considered a hormone, with activation of the vitamin D pro-hormone resulting in the active form, calcitriol, which then produces effects via a nuclear receptor in multiple locations.[4] Cholecalciferol is converted in the liver to calcifediol (25-hydroxycholecalciferol); ergocalciferol is converted to 25-hydroxyergocalciferol. These two vitamin D metabolites (called 25-hydroxyvitamin D or 25(OH)D) are measured in serum to determine a person's vitamin D status.[6][7] Calcifediol is further hydroxylated by the kidneys to form calcitriol (also known as 1,25-dihydroxycholecalciferol), the biologically active form of vitamin D.[8] Calcitriol circulates as a hormone in the blood, having a major role regulating the concentration of calcium and phosphate, and promoting the healthy growth and remodeling of bone. Calcitriol also has other effects, including some on cell growth, neuromuscular and immune functions, and reduction of inflammation.[5]
Vitamin D has a significant role in calcium homeostasis and metabolism. Its discovery was due to effort to find the dietary substance lacking in children with rickets (the childhood form of osteomalacia).[9] Vitamin D supplements are given to treat or to prevent osteomalacia and rickets, but the evidence for other health effects of vitamin D supplementation in the general population is inconsistent.[10][11] The effect of vitamin D supplementation on mortality is not clear, with one meta-analysis finding a small decrease in mortality in elderly people,[12] and another concluding no clear justification exists for recommending supplementation for preventing many diseases, and that further research of similar design is unneeded in these areas.[13]
Mixture of molecular compounds of ergocalciferol with lumisterol, 1:1
Vitamin D2
ergocalciferol (made from ergosterol)
Vitamin D3
cholecalciferol (made from 7-dehydrocholesterol in the skin).
Vitamin D4
22-dihydroergocalciferol
Vitamin D5
sitocalciferol (made from 7-dehydrositosterol)
Several forms (vitamers) of vitamin D exist. The two major forms are vitamin D2 or ergocalciferol, and vitamin D3 or cholecalciferol; vitamin D without a subscript refers to either D2 or D3 or both. These are known collectively as calciferol.[14] Vitamin D2 was chemically characterized in 1931. In 1935, the chemical structure of vitamin D3 was established and proven to result from the ultraviolet irradiation of 7-dehydrocholesterol.[15]
Chemically, the various forms of vitamin D are secosteroids, i.e., steroids in which one of the bonds in the steroid rings is broken.[15] The structural difference between vitamin D2 and vitamin D3 is the side chain of D2 contains a double bond between carbons 22 and 23, and a methyl group on carbon 24.
Biology
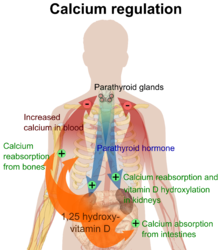
Calcium regulation in the human body.[16] The role of active vitamin D (1,25-dihydroxyvitamin D, calcitriol) is shown in orange.
The active vitamin D metabolite calcitriol mediates its biological effects by binding to the vitamin D receptor (VDR), which is principally located in the nuclei of target cells.[15] The binding of calcitriol to the VDR allows the VDR to act as a transcription factor that modulates the gene expression of transport proteins (such as TRPV6 and calbindin), which are involved in calcium absorption in the intestine.[17] The vitamin D receptor belongs to the nuclear receptor superfamily of steroid/thyroid hormone receptors, and VDRs are expressed by cells in most organs, including the brain, heart, skin, gonads, prostate, and breast.
VDR activation in the intestine, bone, kidney, and parathyroid gland cells leads to the maintenance of calcium and phosphorus levels in the blood (with the assistance of parathyroid hormone and calcitonin) and to the maintenance of bone content.[1]
One of the most important roles of vitamin D is to maintain skeletal calcium balance by promoting calcium absorption in the intestines, promoting bone resorption by increasing osteoclast number, maintaining calcium and phosphate levels for bone formation, and allowing proper functioning of parathyroid hormone to maintain serum calcium levels. Vitamin D deficiency can result in lower bone mineral density and an increased risk of reduced bone density (osteoporosis) or bone fracture because a lack of vitamin D alters mineral metabolism in the body.[18] Thus, vitamin D is also critical for bone remodeling through its role as a potent stimulator of bone resorption.[18]
The VDR regulates cell proliferation and differentiation. Vitamin D also affects the immune system, and VDRs are expressed in several white blood cells, including monocytes and activated T and B cells.[19] In vitro, vitamin D increases expression of the tyrosine hydroxylase gene in adrenal medullary cells, and affects the synthesis of neurotrophic factors, nitric oxide synthase, and glutathione.[20]
Deficiency
Main article: Vitamin D deficiency
A diet deficient in vitamin D in conjunction with inadequate sun exposure causes osteomalacia (or rickets when it occurs in children), which is a softening of the bones. In the developed world, this is a rare disease.[21][22] However, vitamin D deficiency has become a worldwide problem in the elderly and remains common in children and adults.[23][24] Low blood calcifediol (25-hydroxy-vitamin D) can result from avoiding the sun.[25] Deficiency results in impaired bone mineralization and bone damage which leads to bone-softening diseases,[26][27] including rickets and osteomalacia. Being deficient in vitamin D can cause intestinal absorption of dietary calcium to fall to 15%.[1] When not deficient, an individual usually absorbs between 60-80%.[1]
Bone health
Rickets
Main article: Rickets
Rickets, a childhood disease, is characterized by impeded growth and soft, weak, deformed long bones that bend and bow under their weight as children start to walk. This condition is characterized by bow legs,[27] which can be caused by calcium or phosphorus deficiency, as well as a lack of vitamin D; today, it is largely found in low-income countries in Africa, Asia, or the Middle East[28] and in those with genetic disorders such as pseudovitamin D deficiency rickets.[29]
Maternal vitamin D deficiency may cause overt bone disease from before birth and impairment of bone quality after birth.[30][31] Nutritional rickets exists in countries with intense year-round sunlight such as Nigeria and can occur without vitamin D deficiency.[32][33]
Although rickets and osteomalacia are now rare in Britain, outbreaks have happened in some immigrant communities in which osteomalacia sufferers included women with seemingly adequate daylight outdoor exposure wearing Western clothing.[34] Having darker skin and reduced exposure to sunshine did not produce rickets unless the diet deviated from a Western omnivore pattern characterized by high intakes of meat, fish, and eggs, and low intakes of high-extraction cereals.[35][36][37] The dietary risk factors for rickets include abstaining from animal foods.[34][38]
Vitamin D deficiency remains the main cause of rickets among young infants in most countries, because breast milk is low in vitamin D and social customs and climatic conditions can prevent adequate sun exposure. In sunny countries such as Nigeria, South Africa, and Bangladesh, where rickets occurs among older toddlers and children, it has been attributed to low dietary calcium intakes, which are characteristic of cereal-based diets with limited access to dairy products.[37]
Rickets was formerly a major public health problem among the US population; in Denver, where ultraviolet rays are about 20% stronger than at sea level on the same latitude,[39] almost two-thirds of 500 children had mild rickets in the late 1920s.[40] An increase in the proportion of animal protein[38][41] in the 20th century American diet coupled with increased consumption of milk[42][43] fortified with relatively small quantities of vitamin D coincided with a dramatic decline in the number of rickets cases.[1] Also, in the United States and Canada, vitamin D-fortified milk, infant vitamin supplements, and vitamin supplements have helped to eradicate the majority of cases of rickets for children with fat malabsorption conditions.[27]
Osteoporosis and osteomalacia
Main article: Osteoporosis
Main article: Osteomalacia
Osteomalacia is a disease in adults that results from vitamin D deficiency. Characteristics of this disease are softening of the bones, leading to bending of the spine, bowing of the legs, proximal muscle weakness, bone fragility, and increased risk for fractures.[44] Osteomalacia reduces calcium absorption and increases calcium loss from bone, which increases the risk for bone fractures. Osteomalacia is usually present when 25-hydroxyvitamin D levels are less than about 10 ng/mL.[2] Although the effects of osteomalacia are thought to contribute to chronic musculoskeletal pain,[45] there is no persuasive evidence of lower vitamin D levels in chronic pain sufferers[46] or that supplementation alleviates chronic nonspecific musculoskeletal pain.[47]
Skin pigmentation
Dark-skinned people living in temperate climates have been shown to have low vitamin D levels but the significance of this is not certain.[48][49][50] Dark-skinned people may be less efficient at making vitamin D because melanin in the skin hinders vitamin D synthesis.[51]
Non-bone diseases
Mortality, all cause
Use of supplements
The effects of vitamin D supplementation on health are uncertain.[11][52] A 2013 review did not find any effect from supplementation on the rates of disease, other than a tentative decrease in mortality in the elderly.[53] Vitamin D supplements do not alter the outcomes for myocardial infarction, stroke or cerebrovascular disease, cancer, bone fractures or knee osteoarthritis.[54][55] Low vitamin D levels may result from disease rather than cause disease.[53]
A United States Institute of Medicine report states: "Outcomes related to cancer, cardiovascular disease and hypertension, and diabetes and metabolic syndrome, falls and physical performance, immune functioning and autoimmune disorders, infections, neuropsychological functioning, and preeclampsia could not be linked reliably with calcium or vitamin D intake and were often conflicting."[56]:5 Some researchers claim the IOM was too definitive in its recommendations and made a mathematical mistake when calculating the blood level of vitamin D associated with bone health.[57] Members of the IOM panel maintain that they used a "standard procedure for dietary recommendations" and that the report is solidly based on the data. Research on vitamin D supplements, including large-scale clinical trials, is continuing.[57]
Mortality, all-cause
Vitamin D3 supplementation has been tentatively found to lead to a reduced risk of death in the elderly,[12][53] but the effect has not been deemed pronounced or certain enough to make taking supplements recommendable.[13] Other forms (vitamin D2, alfacalcidol, and calcitriol) do not appear to have any beneficial effects with regard to the risk of death.[12] High blood levels appear to be associated with a lower risk of death, but it is unclear if supplementation can result in this benefit.[58] Both an excess and a deficiency in vitamin D appear to cause abnormal functioning and premature aging.[59][60][61] The relationship between serum calcifediol level and all-cause mortality is parabolic.[56] Harm from vitamin D appears to occur at a lower vitamin D level in the black population than in the white population.[56]:435
Bone health
In general, no good evidence supports the commonly held belief that vitamin D supplements can help prevent osteoporosis.[13] Its general use for prevention of this disease in those without vitamin D deficiency is thus likely not needed.[62] For older people with osteoporosis, taking vitamin D with calcium may help prevent hip fractures, but it also slightly increases the risk of stomach and kidney problems.[63] Supplementation with higher doses of vitamin D, in those older than 65 years, may decrease fracture risk.[64] The effect is small or none for people living independently.[65][66] Low serum vitamin D levels have been associated with falls, and low bone mineral density.[67] Taking extra vitamin D, however, does not appear to change the risk.[68] Athletes who are vitamin D deficient are at an increased risk of stress fractures and/or major breaks, particularly those engaging in contact sports. The greatest benefit with supplementation is seen in athletes who are deficient (25(OH)D serum levels <30 ng/mL), or severely deficient (25(OH)D serum levels <25 ng/mL). Incremental decreases in risks are observed with rising serum 25(OH)D concentrations plateauing at 50 ng/mL with no additional benefits seen in levels beyond this point.[69]
Because it found mounting evidence for a benefit to bone health, though it had not found good evidence of other benefits, the US Food and Drug Administration has required manufacturers to declare the amount of vitamin D on nutrition facts labels, as "nutrients of public health significance", since May 2016. By a proposed deadline extension, small manufacturers with less than $10 million in annual food sales will have to comply by 1 Jan 2021, while larger ones have to comply by 1 Jan 2020.[70]
Cancer
Vitamin D supplements have been widely marketed for their claimed anticancer properties.[71] Associations have been shown in observational studies between low vitamin D levels and the risk of development of certain cancers.[72] It is unclear, however, if taking additional vitamin D in the diet or as supplements affects the risk of cancer. Reviews have described the evidence as being "inconsistent, inconclusive as to causality, and insufficient to inform nutritional requirements"[56] and "not sufficiently robust to draw conclusions".[65] One 2014 review found that supplements had no significant effect on cancer risk.[13] Another 2014 review concluded that vitamin D3 may decrease the risk of death from cancer (one fewer death in 150 people treated over 5 years), but concerns with the quality of the data were noted.[73] Insufficient evidence exists to recommend vitamin D supplements for people with cancer, although some evidence suggests that low vitamin D may be associated with a worse outcome for some cancers,[74] and that higher 25-hydroxy vitamin D levels at the time of diagnosis are associated with better outcomes.[75]
Cardiovascular disease
Taking vitamin D supplements does not meaningfully reduce the risk of stroke, cerebrovascular disease, cardial infarction, or ischaemic heart disease.[13] Supplementation may have no effect on blood pressure.[76]
Immune system
Infectious diseases
In general, vitamin D functions to activate the innate and dampen the adaptive immune systems.[77] Deficiency has been linked to increased risk or severity of viral infections, including HIV.[78][79] Low levels of vitamin D appear to be a risk factor for tuberculosis,[80] and historically it was used as a treatment.[81] Supplementation slightly decreases the risk of respiratory tract infections and the exacerbation of asthma.[82][83][84] Evidence is lacking on whether it does so in children under five years of age.[85] No clinical trials have been done to assess its effect on preventing other infections, such as malaria.
Autoimmune diseases
Although tentative data link low levels of vitamin D to asthma, evidence to support a beneficial effect on asthmatics from supplementation is inconclusive.[86] Accordingly, supplementation is not currently recommended for treatment or prevention of asthma.[87] Vitamin D and multiple sclerosis incidence have been linked, but it is not clear what the nature of any causal relationship might be.[88] Two systemic reviews concluded that the evidence for vitamin D supplementation being helpful for treating people with multiple sclerosis is inconclusive.[89][90]
Inflammatory bowel disease
Low levels of vitamin D are associated with two major forms of human Inflammatory bowel disease (IBD): Crohn's disease and ulcerative colitis.[91] However, further studies are required to determine its significance and the potential role of vitamin D axis in IBD.[91][92]
Other conditions
Diabetes -- A systematic review of 2014 concluded that the available studies show no evidence of vitamin D3 supplementation having an effect on glucose homeostasis or diabetes prevention.[93] A review article of 2016 reported that while there is increasing evidence that vitamin D deficiency may be a risk factor for diabetes, over-all evidence regarding vitamin D levels and diabetes mellitus is contradictory, requiring further studies.[94]
Depression -- Clinical trials of vitamin D supplementation for depressive symptoms have generally been of low quality and show no overall effect, although subgroup analysis showed supplementation for participants with clinically significant depressive symptoms or depressive disorder had a moderate effect.[95]
Cognition and dementia -- A systematic review of clinical studies found an association between low vitamin D levels with cognitive impairment and a higher risk of developing Alzheimer's disease. However, lower vitamin D concentrations are also associated with poor nutrition and spending less time outdoors. Therefore, alternative explanations for the increase in cognitive impairment exist and hence a direct causal relationship between vitamin D levels and cognition could not be established.[96]
Pregnancy -- Low levels of vitamin D in pregnancy are associated with gestational diabetes, pre-eclampsia, and small (for gestational age) infants.[97] Although taking vitamin D supplements during pregnancy raises blood levels of vitamin D in the mother at term,[98] the extent of benefits for the mother or baby is unclear.[97][98][99] Pregnant women who take an adequate amount of vitamin D during gestation may experience a lower risk of pre-eclampsia[98] and positive immune effects.[100] A 2018 review found that supplements may reduce the risk of undersized babies and of their poor rate of growth.[101] Pregnant women often do not take the recommended amount of vitamin D.[100]
Weight loss -- Though hypothesized that vitamin D supplementation may be an effective treatment for obesity apart from calorie restriction, one systematic review found no association of supplementation with body weight or fat mass.[102] A 2016 meta-analysis found that circulating vitamin D status was improved by weight loss, indicating that fat mass may be inversely associated with blood levels of vitamin D.[103]
Allowable health claims
Governmental regulatory agencies stipulate for the food and dietary supplement industries certain health claims as allowable as statements on packaging.
European Food Safety Authority
normal function of the immune system[104]
normal inflammatory response[104]
normal muscle function[104]
reduced risk of falling in people over age 60[105]
US Food and Drug Administration
"Adequate calcium and vitamin D, as part of a well balanced diet, along with physical activity, may reduce the risk of osteoporosis."[106]
Health Canada
Adequate calcium and regular exercise may help to achieve strong bones in children and adolescents and may reduce the risk of osteoporosis in older adults. An adequate intake of vitamin D is also necessary[107]
Other possible agencies with claim guidance: Japan FOSHU[108] and Australia-New Zealand.[109]
Dietary intake
Recommended levels
United States
Age group
RDA (IU/day)
(μg/day)[56]
Infants 0–6 months
400*
10
Infants 6–12 months
400*
10
1–70 years
600
15
71+ years
800
20
Pregnant/Lactating
600
15
Age group
Tolerable upper intake level (IU/day)
(µg/day)
Infants 0–6 months
1,000
25
Infants 6–12 months
1,500
37.5
1–3 years
2,500
62.5
4–8 years
3,000
75
9+ years
4,000
100
Pregnant/lactating
4,000
100 [56]
Canada
Age group
RDA (IU)
Tolerable upper intake (IU)[110]
Infants 0–6 months
400*
1,000
Infants 7–12 months
400*
1,500
Children 1–3 years
600
2,500
Children 4–8 years
600
3,000
Children and Adults 9–70 years
600
4,000
Adults > 70 years
800
4,000
Pregnancy & Lactation
600
4,000
Australia and New Zealand
Age group
Adequate Intake (μg)
Upper Level of Intake (μg)[111]
Infants 0–12 months
5*
25
Children 1–18 years
5*
80
Adults 19–50 years
5*
80
Adults 51–70 years
10*
80
Adults > 70 years
15*
80
European Food Safety Authority
Age group
Adequate Intake (μg)[112]
Tolerable upper limit (μg)[113]
Infants 0–12 months
10
25
Children 1–10 years
15
50
Children 11–17 years
15
100
Adults
15
100
Pregnancy & Lactation
15
100
* Adequate intake, no RDA/RDI yet established
Conversion: 1 µg = 40 IU.
Various institutions have proposed different recommendations for the amount of daily intake of vitamin D. These vary according to precise definition, age, pregnancy or lactation, and the extent assumptions are made regarding skin synthesis of vitamin D.[56][110][111][112]
United States
The dietary reference intake for vitamin D issued in 2010 by the Institute of Medicine (renamed National Academy of Medicine in 2015), superseded previous recommendations which were expressed in terms of Adequate Intake. The recommendations were formed assuming the individual has no skin synthesis of vitamin D because of inadequate sun exposure. The reference intake for vitamin D refers to total intake from food, beverages and supplements, and assumes that calcium requirements are being met.[56]:5 The tolerable upper intake level (UL) is defined as "the highest average daily intake of a nutrient that is likely to pose no risk of adverse health effects for nearly all persons in the general population."[56]:403 Although ULs are believed to be safe, information on the long-term effects is incomplete and these levels of intake are not recommended for long-term consumption.[56]:403:433
For U.S food and dietary supplement labeling purposes, the amount in a serving is expressed as a percent of Daily Value (%DV). For vitamin D labeling purposes, 100% of the Daily Value was 400 IU (10 μg), but on May 27, 2016 it was revised to 800 IU (20 μg) to bring it into agreement with the RDA.[114] The deadline to be in compliance was extended to January 1, 2020 for large companies and January 1, 2021 for small companies.[115]
Canada
Health Canada published recommended dietary allowances (RDA) and tolerable upper intake levels for vitamin D in 2012[110] based on the Institute of Medicine report.[56]
Australia and New Zealand
Australia and New Zealand published nutrient reference values including guidelines for dietary vitamin D intake in 2005.[111] About a third of Australians have vitamin D deficiency.[116]
European Union
The European Food Safety Authority (EFSA) in 2016[112] reviewed the current evidence, finding the relationship between serum 25(OH)D concentration and musculoskeletal health outcomes is widely variable. They considered that average requirements and population reference intakes values for vitamin D cannot be derived, and that a serum 25(OH)D concentration of 50 nmol/L was a suitable target value. For all people over the age of 1, including women who are pregnant or lactating, they set an adequate intake of 15 μg/day (600 IU).[112]
The EFSA reviewed safe levels of intake in 2012,[113] setting the tolerable upper limit for adults at 100 μg/day (4000 IU), a similar conclusion as the IOM.
The UK National Health Service recommends babies and young children aged six months to five years, pregnant or breastfeeding women, and sun-deprived elderly people should take daily vitamin supplements to ensure sufficient vitamin D intake.[117] In July 2016, Public Health England recommended that everyone consider taking a daily supplement containing 10 µg of vitamin D during autumn and winter because of inadequate sunlight for vitamin D synthesis.[118]
The Swedish Food Administration recommends a daily intake of 10 μg (400 IU) of vitamin D3 for children and adults up to 75 years, and 20 μg (800 IU) for adults 75 and older.[119]
Non-government organisations in Europe have made their own recommendations. The German Society for Nutrition recommends 20 µg.[120] The European Menopause and Andropause Society recommends postmenopausal women consume15 µg (600 IU) until age 70, and 20 µg (800 IU) from age 71. This dose should be increased to 100 µg (4,000 IU) in some patients with very low vitamin D status or in case of co-morbid conditions.[121]
Sources
Although vitamin D is not present naturally in most foods,[2][4] it is commonly added as a fortification in manufactured foods. In some countries, staple foods are artificially fortified with vitamin D.[122]
Natural sources
Main article: Ergocalciferol § Biosynthesis
In general, vitamin D2 is found in fungi and vitamin D3 is found in animals.[123][124] Vitamin D2 is produced by ultraviolet irradiation of ergosterol found in many fungi. The vitamin D2 content in mushrooms and Cladina arbuscula, a lichen, increase with exposure to ultraviolet light.[125][126] This process is emulated by industrial ultraviolet lamps, concentrating vitamin D2 levels to higher levels.[124]
The United States Department of Agriculture reports D2 and D3 content combined in one value.
Fungal sources
C. arbuscula (lichen), thalli, dry: vitamin D3 0.67 to 2.04 μg/g (27 to 82 IU/g); vitamin D2 0.22-0.55 μg/g (8.8 to 22 IU/g).[125]
Manufactured foods fortified with Vitamin D include some fruit juices and fruit juice drinks, meal replacement energy bars, soy protein-based beverages, certain cheese and cheese products, flour products, infant formulas, many breakfast cereals, and milk.[128][129]
In 2016 in the United States, the Food and Drug Administration (FDA) amended food additive regulations for milk fortification,[130] stating that vitamin D3 levels not exceed 42 IU vitamin D per 100 g (400 IU per US quart) of dairy milk, 84 IU of vitamin D2 per 100 g (800 IU per quart) of plant milks, and 89 IU per 100 g (800 IU per quart) in plant-based yogurts.[131] Plant milks are defined as beverages made from soy, almond, rice, among other plant sources intended as alternatives to dairy milk.
While some studies have found that vitamin D3 raises 25(OH)D blood levels faster and remains active in the body longer,[132][133] others contend that vitamin D2 sources are equally bioavailable and effective as D3 for raising and sustaining 25(OH)D.[124][134][135]
Food preparation
Vitamin D content in typical foods is reduced variably by cooking. Boiled, fried and baked foods retained 69–89% of original vitamin D.[136]
Recommended serum levels
See also: Reference ranges for blood tests § Vitamins, and Hypervitaminosis D § Ethnic differences
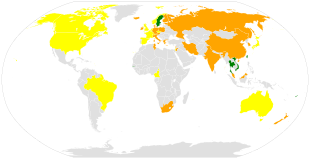
Global vitamin D serum levels among adults (nmol/L).[137][138]
> 75
50-74
25-49
Recommendations on recommended 25(OH)D serum levels vary across authorities, and vary based on factors like age.[5] US labs generally report 25(OH)D levels in ng/mL. Other countries often use nmol/L. One ng/mL is approximately equal to 2.5 nmol/L.
A 2014 review concluded that the most advantageous serum levels for 25(OH)D for all outcomes appeared to be close to 30 ng/mL (75 nmol/L).[139] The optimal vitamin D levels are still controversial and another review concluded that ranges from 30 to 40 ng/mL (75 to 100 nmol/L) were to be recommended for athletes.[140] Part of the controversy is because numerous studies have found differences in serum levels of 25(OH)D between ethnic groups; studies point to genetic as well as environmental reasons behind these variations.[141] Supplementation to achieve these standard levels could cause harmful vascular calcification.[50]
A 2012 meta-analysis showed that the risk of cardiovascular diseases increases when blood levels of vitamin D are lowest in a range of 8 to 24 ng/mL (20 to 60 nmol/L), although results among the studies analyzed were inconsistent.[142]
In 2011 an IOM committee concluded a serum 25(OH)D level of 20 ng/mL (50 nmol/L) is needed for bone and overall health. The dietary reference intakes for vitamin D are chosen with a margin of safety and 'overshoot' the targeted serum value to ensure the specified levels of intake achieve the desired serum 25(OH)D levels in almost all persons. No contributions to serum 25(OH)D level are assumed from sun exposure and the recommendations are fully applicable to people with dark skin or negligible exposure to sunlight. The Institute found serum 25(OH)D concentrations above 30 ng/mL (75 nmol/L) are "not consistently associated with increased benefit". Serum 25(OH)D levels above 50 ng/mL (125 nmol/L) may be cause for concern. However, some people with serum 25(OH)D between 30 and 50 ng/mL (75 nmol/L-125 nmol/L) will also have inadequate vitamin D.[56]
Excess
Further information: hypervitaminosis D
Vitamin D toxicity is rare.[24] It is caused by supplementing with high doses of vitamin D rather than sunlight. The threshold for vitamin D toxicity has not been established; however, according to some research, the tolerable upper intake level (UL) is 4,000 IU/day for ages 9–71[143] (100 µg/day), while other research concludes that, in healthy adults, sustained intake of more than 1250 μg/day (50,000 IU) can produce overt toxicity after several months and can increase serum 25-hydroxyvitamin D levels to 150 ng/mL and greater.[24][144] Those with certain medical conditions, such as primary hyperparathyroidism,[145] are far more sensitive to vitamin D and develop hypercalcemia in response to any increase in vitamin D nutrition, while maternal hypercalcemia during pregnancy may increase fetal sensitivity to effects of vitamin D and lead to a syndrome of mental retardation and facial deformities.[145][146]
A review published in 2015 noted that adverse effects have been reported only at 25(OH)D serum concentrations above 200 nmol/L.[140]
Published cases of toxicity involving hypercalcemia in which the vitamin D dose and the 25-hydroxy-vitamin D levels are known all involve an intake of ≥40,000 IU (1,000 μg) per day.[145]
Pregnant or breastfeeding women should consult a doctor before taking a vitamin D supplement. The FDA advised manufacturers of liquid vitamin D supplements that droppers accompanying these products should be clearly and accurately marked for 400 international units (1 IU is the biological equivalent of 25 ng cholecalciferol/ergocalciferol). In addition, for products intended for infants, the FDA recommends the dropper hold no more than 400 IU.[147] For infants (birth to 12 months), the tolerable upper limit (maximum amount that can be tolerated without harm) is set at 25 μg/day (1,000 IU). One thousand micrograms per day in infants has produced toxicity within one month.[144] After being commissioned by the Canadian and American governments, the Institute of Medicine (IOM) as of 30 November 2010[update], has increased the tolerable upper limit (UL) to 2,500 IU per day for ages 1–3 years, 3,000 IU per day for ages 4–8 years and 4,000 IU per day for ages 9–71+ years (including pregnant or lactating women).[143]
Calcitriol itself is auto-regulated in a negative feedback cycle, and is also affected by parathyroid hormone, fibroblast growth factor 23, cytokines, calcium, and phosphate.[148]
Effect of excess
Vitamin D overdose causes hypercalcemia, which is a strong indication of vitamin D toxicity – this can be noted with an increase in urination and thirst. If hypercalcemia is not treated, it results in excess deposits of calcium in soft tissues and organs such as the kidneys, liver, and heart, resulting in pain and organ damage.[24][27][44]
The main symptoms of vitamin D overdose which are those of hypercalcemia including anorexia, nausea, and vomiting. These may be followed by polyuria, polydipsia, weakness, insomnia, nervousness, pruritus and ultimately renal failure. Furthermore, proteinuria, urinary casts, azotemia, and metastatic calcification (especially in the kidneys) may develop.[144] Other symptoms of vitamin D toxicity include mental retardation in young children, abnormal bone growth and formation, diarrhea, irritability, weight loss, and severe depression.[24][44]
Vitamin D toxicity is treated by discontinuing vitamin D supplementation and restricting calcium intake. Kidney damage may be irreversible. Exposure to sunlight for extended periods of time does not normally cause vitamin D toxicity. The concentrations of vitamin D precursors produced in the skin reach an equilibrium, and any further vitamin D produced is degraded.[145]
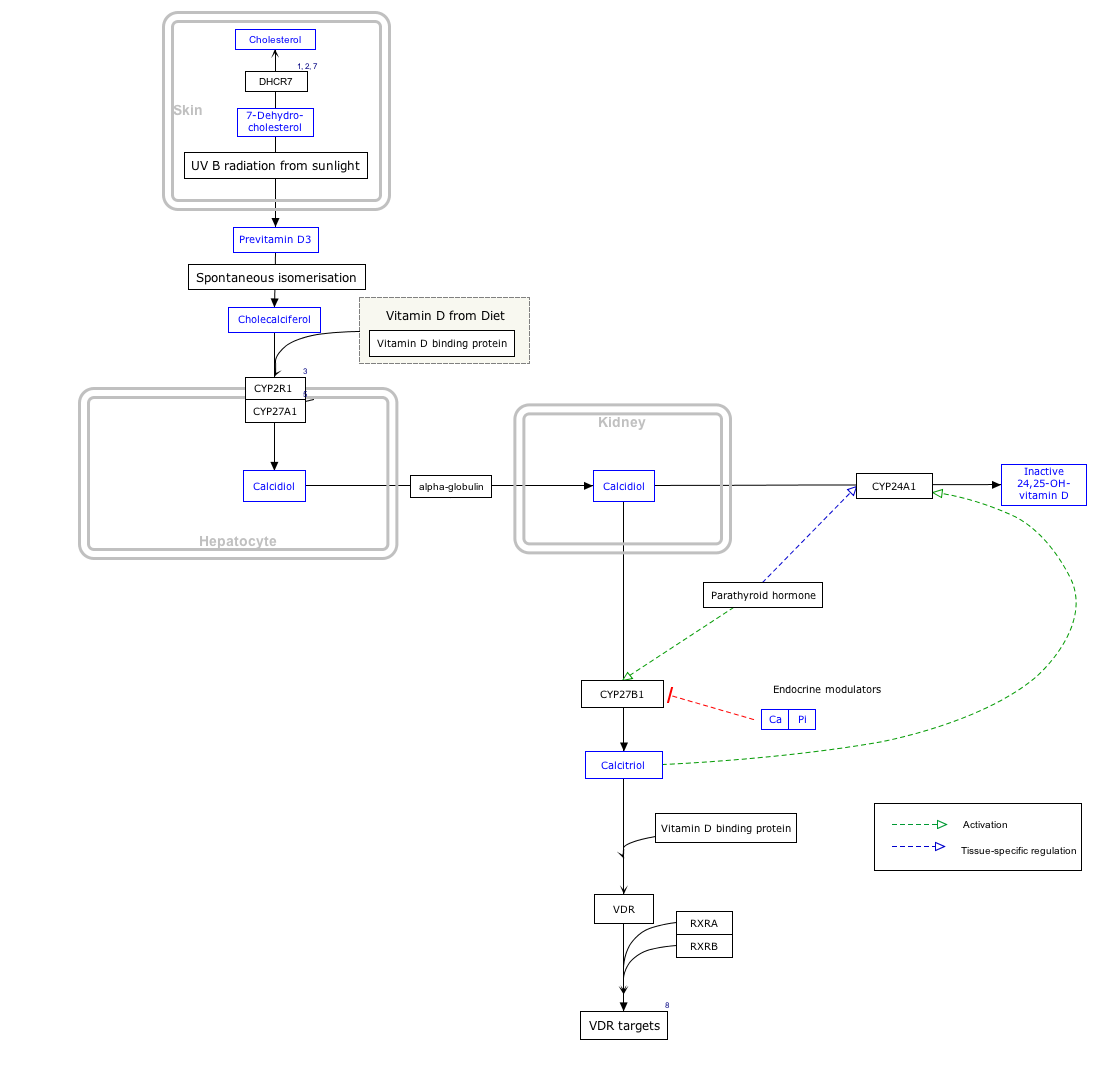
Biosynthesis
Synthesis of vitamin D in nature is dependent on the presence of UV radiation and subsequent activation in liver and in kidney. Many animals synthesize vitamin D3 from 7-dehydrocholesterol, and many fungi synthesize vitamin D2 from ergosterol.[123][124]
Interactive pathway
Click on icon in lower right corner to open. Click on genes, proteins and metabolites below to link to respective articles.[§ 1]
EastEnders character This article is about the soap opera character. For the British tennis player, see Peggy Michell. For the author, see Margaret Mitchell. Peggy Mitchell Barbara Windsor as Peggy Mitchell (2008) EastEnders character Portrayed by Jo Warne (1991) Barbara Windsor (1994–2016) Duration 1991, 1994–2010, 2013–2016 First appearance Episode 650 30 April 1991 ( 1991-04-30 ) Last appearance Episode 5286 17 May 2016 ( 2016-05-17 ) (appearance) Episode 5287 19 May 2016 (voiceover) Introduced by Michael Ferguson (1991) Barbara Emile (1994) Louise Berridge (2004) Kate Harwood (2005) Lorraine Newman (2013) Dominic Treadwell-Collins (2014) Spin-off appearances The Mitchells - Naked Truths (1998) Classification Former; regular Profile Other names Peggy Butcher Occupation Barmaid Businesswoman Pub landlady Jo Warne as Peggy Mitchell (1991) Family Family Mitchell Father Jack Martin Mother Lily Martin Sisters Aunt ...
The Forum "LA Forum" Prairie Ave. façade of The Forum in 2014 Full name The Forum, presented by Chase Former names The Forum (1967–1988) Great Western Forum (1988–2003) Address 3900 W. Manchester Blvd Location Inglewood, California Coordinates Coordinates: 33°57′29″N 118°20′31″W / 33.95806°N 118.34194°W / 33.95806; -118.34194 Public transit Downtown Inglewood station Owner The Madison Square Garden Company Operator MSG Entertainment Seating type Reserved Capacity 17,500 Half-bowl: 8,000 Construction Broke ground July 1, 1966 ( 1966-07-01 ) Opened December 30, 1967 ( 1967-12-30 ) Renovated 1988, 2012–2014 Construction cost $16 million Renovation: 2014: $76.5 million Architect Charles Luckman Associates (original) Brisbin Brook Beynon (renovation) Structural engineer Johnson & Nielsen Associates (original) Severud Associates (renovation) Genera...
Palaiologos Παλαιολόγος Palaeologus, Palaeologue Imperial Family Double-headed eagle with the family cypher Country Byzantine Empire, Duchy of Montferrat (remaining lineage after Empire annexed by Ottomans) Founded 11th century ( 11th century ) Founder Nikephoros Palaiologos (first known) Final ruler Constantine XI Palaiologos (Byzantine Empire) Margaret Paleologa (Montferrat) Titles Byzantine Emperor Marquess of Montferrat Style(s) "Augustus" "Basileus" "Autokrator" Traditions Greek Orthodoxy (predominantly) Roman Catholicism (remaining lineage in Montferrat) Dissolution 1533 ( 1533 ) Cadet branches Claimants: House of Kastrioti (defunct) House of Rurik (defunct) Palaiologan dynasty Chronology Michael VIII 1259–1282 with Andronikos II as co-emperor, 1261–1282 Andronikos II 1282–1328 with Michael IX (1294–1320) and Andronikos III (1321–1328) as co-emperors Andronikos III 1328–1341 John...